Childhood brain and spinal cord diseases require completely different clinical approaches than those for adults because they affect the nervous system, which is in a dynamic development process.
Conditions such as hydrocephalus, in particular, can cause developmental delays by creating permanent pressure on brain tissue if not detected early.
Pediatric neurosurgery expertise necessitates both surgical technical skill and a vision that preserves the child’s growth potential during this sensitive process.
Today, thanks to microsurgery and endoscopic methods, high success rates and improved quality of life are observed in the management of these complex diseases.
What is Childhood Hydrocephalus? Causes and Mechanism of Formation
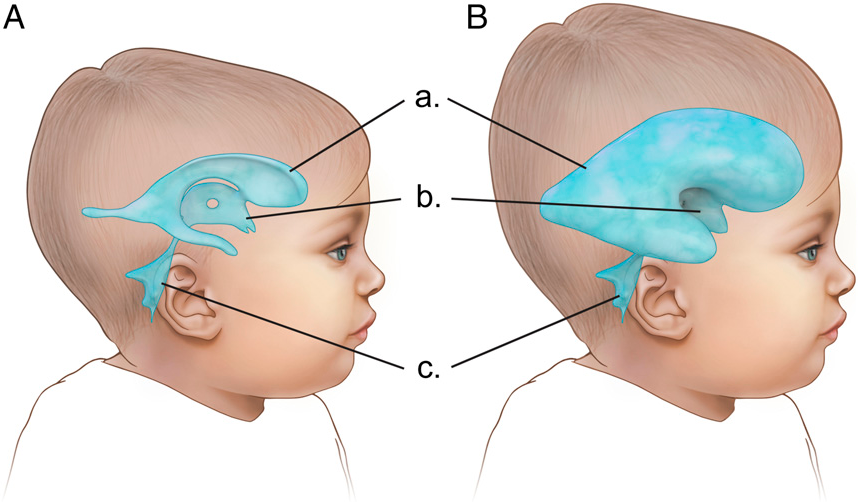
Hydrocephalus is an increase in intracranial pressure resulting from the accumulation of excessive amounts of cerebrospinal fluid (CSF) in the brain cavities (ventricles).
Under normal conditions, CSF is produced in the brain, circulates through channels, and is then reabsorbed into the bloodstream.
A disruption in this balance at any stage of production, circulation, or absorption causes the fluid to become trapped in the ventricles.
Cerebrospinal Fluid (CSF) Circulation and Types of Obstruction
CSF circulation plays critical roles such as cushioning, nourishment, and waste removal.
If the fluid cannot progress through the narrow channels between the ventricles (e.g., the Sylvian aqueduct) due to a physical obstruction, this is called “obstructive” (blockage-type) hydrocephalus.
If the fluid passes through the channels but has problems at the absorption point, a “communicating” hydrocephalus pattern emerges.
Differences Between Congenital (Present at Birth) and Acquired Hydrocephalus
Congenital hydrocephalus occurs while the baby is still in the womb due to genetic factors or developmental anomalies.
Acquired hydrocephalus develops after birth as a result of meningitis, brain hemorrhage (especially in premature babies), or masses.
Symptoms of Hydrocephalus in Infants and Children
Symptoms vary depending on the child’s age group and the fusion status of the skull bones.
Physical Findings and Head Circumference Monitoring in Infancy
Since the skull bones in infants have not yet fused, the most prominent sign is rapid growth of the head circumference deviating from the percentile curves.
Tension in the fontanelle, visible veins on the scalp, and the infant’s inability to lift their eyes from down to up (sunset sign) are findings that require urgent evaluation.
Neurological Symptoms and Visual Impairments in School-Age Children
In older children, head growth is not observed because the skull bones have fused, but increased intracranial pressure causes severe headaches and vomiting.
Symptoms such as imbalance, double vision, sudden decline in school performance, and urinary incontinence may be signs of a hidden hydrocephalus.
Diagnostic Methods in Pediatric Brain and Spinal Cord Diseases
Modern diagnostic tools play a fundamental role in clarifying surgical decisions and risk analysis.
Transfontanellar Ultrasonography: The Radiation-Free First Step in Infants
In infants whose fontanelle has not yet closed, the width of the ventricles can be quickly checked using radiation-free ultrasonography.
This method is particularly convenient for bedside monitoring of brain hemorrhage and hydrocephalus in premature infants.
Safety in Pediatric MRI and CT Imaging Techniques
MRI (Magnetic Resonance Imaging) is the gold standard for showing nerve tissue in the finest detail; however, sedation may be necessary to prevent movement during the scan in young children.
CT (Computed Tomography) provides rapid results in emergency situations, but it should be performed using “pediatric protocols” that optimize radiation dose in children.
Modern Surgical Options in Hydrocephalus Treatment
The treatment method is selected based on the type of hydrocephalus and the underlying cause.
Shunt Surgery: Ventriculoperitoneal (VP) Shunt Application
A shunt is a one-way valve system that drains excess fluid from the brain into the abdominal cavity.
This tube system is placed under the skin so that it is not visible from the outside of the body.
Adjustable valves used in current technology allow us to change the flow rate of fluid after surgery without the need for surgery, using an external magnet.
Endoscopic Third Ventriculostomy (ETV): Shunt-Free Treatment Option
Particularly in hydrocephalus cases caused by blockages, a new window is opened to allow fluid to flow through its natural circulation pathways by entering the brain with an endoscopic camera.
The main advantage of this method is that no foreign object, such as a shunt, is placed in the patient’s body.
Shunt Revision and Infection Management
Shunts can become blocked or infected over time; this condition is called “shunt dysfunction.”
Although these risks are minimized with surgical precision and modern antibiotic-coated shunt systems, regular check-ups are vital.
Pediatric Brain Surgery Treatment Comparison Table
| Treatment Method | Purpose of Application | Advantages | Recovery Time | Long-Term Risk |
| VP Shunt | All types of hydrocephalus | Wide range of applications | 1 Week | Obstruction/Infection |
| Endoscopic VENT | Obstructive hydrocephalus | No foreign bodies | 3-5 Days | Risk of closure |
| Microsurgery | Tumor and cyst treatment | Definite tissue diagnosis | 2-4 weeks | Neurological risks |
| Spina Bifida Repair | Spinal cord defect | Protects nerve tissue | 4 weeks | Tight spinal cord |
Childhood Spinal Cord Disorders and Spina Bifida
Openings resulting from the spinal cord failing to complete its development in the womb are serious conditions requiring immediate intervention after birth.
Repair of Meningomyelocele and Congenital Spinal Defects
Microsurgical repair performed within the first 48 hours after birth prevents meningitis by cutting off the nerves’ contact with the external environment.
The primary goal of these operations is to anatomically reposition the nerve roots and minimize functional loss.
Tethered Cord Syndrome Surgery (Tethered Cord Release)
As the child grows, the spinal cord, which cannot adapt to the elongation of the spine and remains tethered below, stretches and causes nerve damage.
Microsurgical detethering of the nerve can prevent future problems such as paralysis and urinary incontinence.
Prof. Dr. Erdinç Özek
“In pediatric brain surgery, timing is as much an art as surgical technique. When performing surgery on a baby’s brain, we plan not only to solve the immediate problem, but also to ensure that child’s academic success and motor skills 20 years down the line. I understand parents’ fear of ‘shunts’; however, with the right technology and experience, these systems are the safest haven for ensuring a child lives a normal life.”
Childhood Brain Tumors and Microsurgical Treatment
The biology of childhood tumors differs from that of adults, and they are usually located in the posterior fossa (the cerebellar region) of the brain.
Use of Neuromonitoring in Pediatric Oncological Surgery
Neuro-monitoring technology, which tracks electrical signals passing through nerves during surgery, minimizes the risk of damaging healthy tissue while removing the tumor.
This technology allows the surgeon to operate within a “safe zone.”
The Importance of Postoperative Neurological Rehabilitation
The brain’s ability to recover (plasticity) after surgery is very high in children.
Physical therapy and special education support are the most important factors in accelerating functional recovery after surgery.
Surgery Process and Recovery Guide for Families
After the surgical decision, the family’s greatest concern is the preparation and hospital process.
Preoperative Preparation and Anesthesia Process
Under the supervision of pediatric anesthesiologists, medication protocols specific to the child’s age and weight are prepared.
The preoperative fasting period and psychological preparation (play therapy support, etc.) ensure that the process is trauma-free.
Long-Term Follow-Up: Shunt Checks and Developmental Monitoring
Children who have undergone hydrocephalus or brain tumor surgery should be regularly monitored in terms of developmental milestones.
Annual MRI checks and periodic neurological examinations ensure the early detection of a possible recurrence or shunt problem.
Anonymous Case Example
A baby diagnosed with ventricular enlargement at 32 weeks in utero was brought to our clinic in the second week after birth due to excessive head growth.
Examinations revealed severe hydrocephalus, and an adjustable valve VP shunt system was implanted.
After surgery, the baby’s head growth stopped and motor development returned to normal. At the 4-year checkup, the baby showed completely age-appropriate development, and the shunt setting was optimized with a single external intervention.
You may need scientifically based guidance for all your questions regarding your child’s brain and spinal cord health.
With accurate diagnosis and microsurgical techniques, promising outcomes are achievable even in the most complex cases.
For detailed information, you can consult an expert and schedule an appointment at our clinic.
Frequently Asked Questions
Will a child diagnosed with hydrocephalus have normal intellectual development?
In children diagnosed early and whose fluid pressure on the brain is controlled in time through surgical methods, intellectual and cognitive development can continue in complete harmony with their peers, provided that the brain tissue does not suffer permanent damage.
Is the shunt system visible from the outside?
Since all parts of the shunt system are placed under the skin, it is not visible from the outside; only in weak babies, the valve mechanism behind the ear and the thin line in the neck area may be felt as a slight bulge, but this appearance disappears as the child grows.
How can we tell if the shunt is blocked or malfunctioning?
Sudden onset of projectile vomiting, severe headache, constant drowsiness, restlessness, or regression in previously acquired skills (such as walking or talking) are serious warning signs that the shunt is not working and require urgent consultation with a neurosurgeon.
Is there a risk of shunt rupture in children who participate in sports?
Shunt systems are made of highly flexible and durable materials and are not damaged during daily activities; however, direct blows to the head during karate, boxing, or other high-impact contact sports involving violent collisions can damage the mechanism, so it is recommended to avoid such sports.
Can endoscopic ETV surgery be performed on every hydrocephalus patient?
The ETV method is particularly successful in cases where there is a physical obstruction in the intracranial channels (such as aqueduct stenosis); however, in patients with problems at the absorption points of the cerebrospinal fluid or who have previously had severe meningitis, the chances of success are low, so shunt treatment is preferred in these cases.
Can children who have undergone surgery continue their normal school life?
Children who have completed the treatment process and have regular check-ups can continue their normal education, play with their friends, and experience no restrictions in terms of academic achievement, provided that no physical or mental disabilities have developed.
Scientific References
PubMed / NCBI: “Pathophysiology and management of pediatric brain tumors”. https://pubmed.ncbi.nlm.nih.gov/30562341/
Neurosurgical Focus: “Innovations in pediatric neuro-oncology and surgical techniques”. https://thejns.org/focus/view/journals/neurosurg-focus/48/1/article-pE1.xml
